

They Are Caused By A Co-Infection
A PREVALENT BUT UNMENTIONED MEGA-VIRUS APPEARS TO CAUSE THE HOSPITALIZATIONS & DEATHS THAT ARE ATTRIBUTED TO
COVID-19 CORONAVIRUS?
And Guess Who Is Developing A Vaccine For This Overlooked Virus?
In an unprecedented era of vaccine propaganda, medical misinformation, false-positive nasal swab PCR tests, problematic spike protein vaccines that don’t halt infection or transmission, and questionable preventive measures (face masks, social distancing), scientific scrutiny has yet to fully explain why even a laboratory made gain-of-function virus strikes so hard against elderly adults.
Most of the deaths attributed to Covid-19 coronavirus infection occur among very old, infirm, fragile, morbid subjects. But why this coronavirus over other viruses? Maybe there is an overlooked answer to that question.
The ubiquitous but overlooked virus
A largely unmentioned virus that is innocuous (usually symptomless and dormant) but ubiquitous (present but dormant in most people), which represents co-infection, appears to be what has caused most of the hospitalizations and deaths reported for aged adults with COVID-19 coronavirus infection.
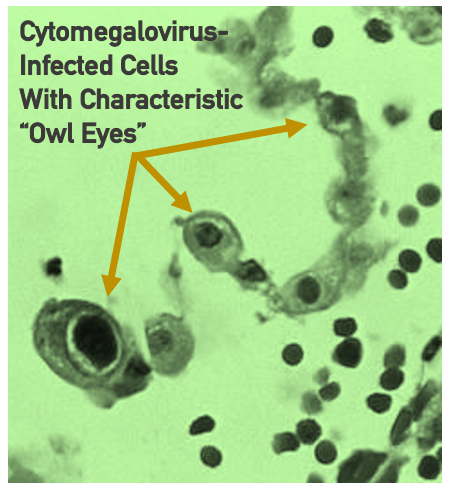
This virus ends up infecting cells that look overly large (mega-sized). It is called cyto (cell) megalo (overly large) virus or cytomegalovirus (CMV). It is unique to humans, not animals.
NO vaccine and guess who is making one?
There is no approved vaccine for this virus. And guess which vaccine maker is in Stage 3 Clinical Trials for possibly the first vaccine against this often-quiescent virus that causes birth defects if it erupts in birthing mothers and induces death among older or immune-compromised adults?
The same criminal company that makes a toxic, Nuremberg Code-violating, worse-than-the-coronavirus RNA spike-protein vaccine! Yep, it’s them, again. The experimental vaccine is comprised of six RNAs that target two proteins on the surface of cytomegalovirus.
And will this vaccine maker be operating under the same contrived emergency declaration that was called for COVID-19, that waived informed consent requirements and resulted in Americans having a vaccine forced upon them? Will this vaccine be forced on human populations it lives in a dormant form most of people’s lives? God only knows once politicians get a hold of it.
Most people will be exposed to cytomegalovirus (CMV) over their lifetime.
Dormant cytomegalovirus is carried by 70-90% of the adult population and is reactivated by inflammation. One third of patients in hospital intensive care units reactivate CMV which doubles their mortality rate!
An aging factor called cell senescence results in weakened white blood cells (neutrophils, natural killer cells, macrophages). CMV infection hastens senescence of immune cells. CMV is said to accelerate the aging of naïve T-cells by 20 years.
There is agreement that Covid-19 co-infection with cytomegalovirus is associated with higher rates of mortality in older people who have an aged (senescent) immune system.
So-called naïve T-cells (T-cells that are not yet programmed to generate memory immunity), produced in abundance in the thymus gland when young, are reduced by 99% in numbers in adults over age 70. The combined senescence of T-cells plus co-infection of Covid-19 coronavirus and cytomegalovirus may be too much to overcome in aged subjects.
There is a dramatic decline in T-cells in Covid-19 patients, particularly CD8 T-cells. CMV-induced immune suppression among senior adults may increase the risk of dying from influenza or other infectious diseases as well.
CMV infection increases severity of illness
Initial CMV infection, usually in youth, produces mild or no symptoms. However, CMV co-infection is reported to increase severity and associated blood clotting among adults which have been reported with Covid-19. The difference between mild and severe Covid-19 cases may be reactivation of CMV.
CMV is not thought to cause any illness in healthy younger-aged adults unless reactivated by inflammation, such as among organ transplant patients who are given immune suppressant anti-rejection drugs.
CMV is reactivated in 30-35% of ICU COVID-19 patients which doubles their mortality rate.
Massive infiltration of white blood cells called macrophages into the lungs may carry dormant CMV that may be reactivated by Covid-19 itself.
Two life-threatening factors, overactivation of the immune system and blood clotting, are now linked to CMV.
Doctors usually don’t look for CMV infection
The diagnosis of CMV is easily missed in the ICU.
In a study of ICU Covid-19 patients co-infected with CMV, 50% showed reactivation of CMV. In another study 82% of patients experienced reactivation of CMV after admission to the ICU for Covid-19 infection.
Critical T-cells
White blood cells produce long-term memory immunity. In older adults cytomegalovirus infection is more destructive to T-cell counts than aging itself.
Over a lifetime more and more T-cells are devoted to targeting CMV, leaving the body vulnerable to other threats.
In a study of 26 patients (age 66-80 years) Covid-19 patients with negative CMV tests upon admission to the ICU, 6 of 26 (23%) developed CMV infection during mechanical ventilation, and ventilation lasted longer in the CMV-positive group (40.5 days compared to the non-CMV group (18.0 days). Two of six died in the CMV group versus none in the non-CMV group.
At the writing of this report there are no approved vaccines for CMV. Nor are there non-problematic antiviral drugs.
Antidote: resveratrol
It seems like the antidote to everything that ails mankind is resveratrol these days.
This red wine molecule is known as a powerful activator of the Sirtuin1 survival gene. Resveratrol inhibits replication of cytomegalovirus in infected lung cells.
To the contrary, cytomegalovirus infection shuts off the Sirtuin1 gene and therefore facilitates abnormal new blood vessel growth (called angiogenesis) which occurs among patients with macular degeneration, diabetic retinopathy and metastatic (spreading) cancer. So CMV infection could be very deleterious to people with these chronic or acute problems.
In fact, CMV infection was found among 55% of patients with the invasive and fast-progressive form of macular degeneration, 39% of the CMV-infected patients with the slow-form of macular degeneration and only among 34% of healthy control subjects.
Cytomegalovirus and vitamin D
Vitamin D, the sunshine vitamin, is an essential nutrient/hormone that tunes up the immune system. Vitamin D is produced in the skin (as vitamin D3 cholecalciferol), stored in the liver (as calcidiol) and converted to its active form (calcitriol) in the kidneys. Cytomegalovirus does not interfere with any of these forms of vitamin D.
However, once the active form of vitamin D (calcitriol) is released from the kidneys it enters living cells via a doorway called the vitamin D receptor. Of all things, cytomegalovirus dulls this receptor for the active form of vitamin D to enter cells. Flu or cold viruses do not interfere with the vitamin D cell receptor. But cytomegalovirus certainly does. Vitamin D (as calcitriol) is then unable to inhibit CMV replication.
Of note, resveratrol binds to and activates the vitamin D receptor.
This may explain why there are some disappointing vitamin D studies in humans. Cells in the body may not be able to respond to vitamin D or sunshine due to blockage at the cell receptor.
Iron requirement for cytomegalovirus cell enlargement
Viruses are not alive and must hijack and enter living cells in order to replicate. CMV-infected cells are by definition abnormally enlarged cells as depicted in a graphic accompanying this report.
Iron is required for CMV cell enlargement. Therefore, it is no surprise to learn that iron binders/chelators (key-late-ors) have been found to be inhibit CMV cell enlargement.
Natural iron binders such as IP6 (phytic acid) extracted from rice bran and quercetin from red apple peel or red onions may be useful for CMV-infected individuals to halt eruption.
Lysine/arginine balance and control of Covid-19 and CMV
In the 1960s it was widely reported that herpes-class viruses depend upon the amino acid arginine to replicate. It wasn’t till 1974 that Dr. Christopher Kagan reported that the amino acid lysine counters the herpes replication induced by arginine. Surprisingly, over 40 years later, Kagan, Chaihorsky and colleagues reported that lysine/arginine balance also abolishes Covid-19 infections.
Given that CMV is a herpes family virus, is it also kept in a dormant state by lysine? A forgotten report published in the 1970s suggest it is. Cytomegalovirus replication is also strongly dependent upon arginine.
While no medication has been authorized for the control of Covid-19 or cytomegalovirus other than problematic and often ineffective anti-viral drugs, this well-established science suggests both Covid-19 and CMV could be quelled with a simply inexpensive amino acid.
Dietary control would also be of importance. Preference of lysine-rich foods (cheese, eggs, chicken) and avoidance of arginine-rich foods (chocolate, nuts, seeds, spinach) would be preventive.
Suggestions for action:
- Lysine abolishes herpes (including shingles, chicken pox, lip cold sores, Bell’s palsy and cytomegalovirus), and Covid-19 corona virus and is widely available as an inexpensive dietary supplement. Theoretically lysine would work to prevent infection and transmission, something Covid-19 vaccines don’t do. Consumption of virus-activating arginine-rich foods (chocolate, nuts) should be avoided during active infection, and lysine-rich foods (cheese, turkey, chicken) consumed.
- Resveratrol is a widely available dietary supplement when taken in modest doses (no more than 250 milligrams) and inhibits cytomegalovirus replication and aids vitamin D entry into cells via the vitamin D receptor. Resveratrol also inhibits blood clots associated with Covid-19 infection.
- Iron chelators such as quercetin and IP6 rice bran halt growth of cytomegalovirus and characteristic cell enlargement. Both are widely available as dietary supplements.
- This report suggests the ability to keep cytomegalovirus in check, in its dormant state, means coronavirus infection is not likely to become acute and result in hospitalization or death. Individuals with prior herpes infections may be wise to continually supplement with lysine.
- Current vaccines don’t protect against cytomegalovirus.
- These remedies are scientifically sound, do not induce significant side effects, are economical, yet the medical establishment has chosen to keep knowledge of these remedies from the public and allow patients to experience needless acute viral infections, hospitalizations and death.

