

Not only are we faced with aggressive attempts to force us into participating in a recklessly dangerous COVID-19 mass vaccination experiment, mainstream media are now drumming up concerns about the next flu season on top of it. As reported by NBC News:1
“More than a year after the pandemic started, Covid-19 is still ravaging parts of the world, but now scientists are warning that another virus could be a serious threat in the coming months: influenza.
This season, the flu virtually disappeared, with less than 2,000 lab-confirmed cases in the United States to date, according to the Centers for Disease Control and Prevention.2 In a typical flu season, the U.S. could see more than 200,000 lab-confirmed cases by this time of year, a tiny fraction of the true number of cases, estimated to range from 9 million to 45 million annually …
According to scientists like Dr. Andy Pekosz, a professor of microbiology at the Johns Hopkins Bloomberg School of Public Health, a year without much flu could lead to a year with a whole lot of flu.
‘We’ve gone over a year without a significant portion of the population getting infected with flu and getting immunity because of that,’ Pekosz said. ‘That could mean that the susceptible people in the population to flu are going to be increasing.’”
Did Masks and Social Distancing Eliminate Influenza?
According to NBC News,3 COVID-19 mitigation measures such as universal mask wearing, social distancing and lockdowns prevented transmission of influenza during the 2020/2021 season. Well, as the old saying goes, “If you believe that, I’ve got a bridge to sell you.”
First of all, the idea that masks and social distancing magically eradicated influenza, not just in the U.S. but around the world,4 is not supported by any serious science on masks, most of which actually looked at flu viruses. I’ll review some of those below.
It’s also implausible for the simple fact that COVID-19 statistics on cases, hospitalizations and mortality were all massively manipulated. There’s simply no telling how many so-called COVID-19 cases, hospitalizations and probably even deaths, were actually flu-related.
Everyone, everywhere was being tested for COVID-19. Not influenza. And anyone presenting flu-like symptoms was automatically assumed to have COVID-19. Even if the flu was tested for and was positive, any falsely positive COVID test would change the diagnosis from flu to COVID-19.
Granted, each year, one particular strain of influenza virus will tend to predominate (but will vary from region to region), but it’s never 100% just one strain. So, the likelihood of virtually all infections this past year being due to SARS-CoV-2 is ridiculously small to say the least.
Lastly, if masks and social distancing worked like magic to prevent the spread of influenza, why did these measures not eradicate SARS-CoV-2? You simply cannot have it both ways. Masking and social distancing could not possibly have prevented influenza while simultaneously having no measurable impact on COVID-19.
We’ve Long Known Masks Don’t Work Against Flu
The available research has been rather consistent: Mask wearing does not reduce the prevalence of viral upper respiratory illness, and a vast majority of these studies looked at influenza specifically. For example, a policy review paper5 published in Emerging Infectious Diseases in May 2020, which looked at 10 randomized controlled trials, found there was “no significant reduction in influenza transmission with the use of face masks.”
In 2019, a review of interventions for flu epidemics published by the World Health Organization concluded the evidence for face masks was slim, and what little benefit there was might simply be due to chance:6
“Ten relevant RCTs were identified for this review and meta-analysis to quantify the efficacy of community-based use of face masks …
In the pooled analysis, although the point estimates suggested a relative risk reduction in laboratory-confirmed influenza of 22% in the face mask group, and a reduction of 8% in the face mask group regardless of whether or not hand hygiene was also enhanced, the evidence was insufficient to exclude chance as an explanation for the reduced risk of transmission.”
Similarly, a 2020 guidance memo by the WHO pointed out that:7
“At present, there is no direct evidence … on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19.”
A meta-analysis and scientific review8 led by respected researcher Thomas Jefferson, cofounder of the Cochrane Collaboration, posted on the prepublication server medRxiv in April 2020, found that, compared to no mask, mask wearing in the general population or among health care workers did not reduce influenza-like illness cases or influenza.
In one study, which looked at quarantined workers, it actually increased the risk of contracting influenza, but lowered the risk of influenza-like illness. They also found there was no difference between surgical masks and N95 respirators.
A similar finding was reported in a 2009 study,9 which compared the effectiveness of surgical masks and N95 respirators to prevent seasonal influenza in a hospital setting; 23.6% of the nurses in the surgical mask group still got the flu, as did 22.9% of those who wore N95 respirators.
Seeing how we’ve been encouraged to use cloth masks, it’s worth noting that research10 published in 2015 actually found health care workers who wore cloth masks had a 72% higher rate of lab-confirmed respiratory virus infections, compared to those wearing medical masks or controls (who used standard practices that included occasional medical mask wearing).
According to the authors, “the results caution against the use of cloth masks … Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.”
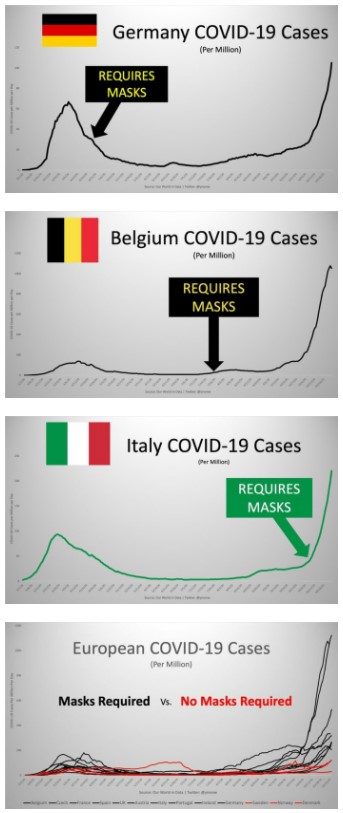
Mask Mandates Had No Impact on COVID-19
COVID-19 statistics also defy the idea that masks made any difference. In his article,11 “These 12 Graphs Show Mask Mandates Do Nothing to Stop COVID,” bioengineer Yinon Weiss points out that “No matter how strictly mask laws are enforced nor the level of mask compliance the population follows, cases all fall and rise around the same time.”
To see all of the graphs, check out Weiss’ article.12 Here are just a select few to bring home the point:
Social distancing, meanwhile, at best only led to a plateau in infectious spread, according to researchers at the University of Rochester and Cornell University,13 while lockdowns had a net negative effect.14 According to a report15 by Canadian pediatric infectious disease specialist Dr. Ari Joffe, lockdown harms are about 10 times greater than the benefits.
Coming Next: Gene-Based Combo Shots
As detailed in “How COVID Vaccines Can Cause Blood Clots and More,” the gene-based COVID-19 “vaccines” are a disaster in the making. As of May 14, 2021, the U.S. Vaccine Adverse Event Reporting System (VAERS) had logged 227,805 adverse events following COVID vaccination, including 4,201 deaths and 18,528 serious injuries.16
This included 293 injuries among 12- to -17-year-olds, 23 of which were rated serious. Of the deaths, two were under the age of 16, 23% occurred within 48 hours of vaccination and 20% were due to cardiac disorders. And remember, only 1% to 10% of adverse effects and deaths are reported to VAERS, so the real-world number of deaths could range from 42,000 to 420,000.
In a recent interview with Stephanie Seneff, Ph.D., and Judy Mikovits, Ph.D., we reviewed several of the ways in which these vaccines destroy your health. Importantly, it’s been fairly well-established that the primary damage in COVID-19 is caused by the spike protein, and this is what these vaccines are programming your body to produce.
Despite there being very obvious problems with this technology, vaccine scientists are moving full steam ahead to produce several additional gene-based vaccines, including:
•The first COVID-flu RNA vaccine17 — This combo vaccine is currently being tested on ferrets. The vaccine, made by NovaVax, combines NanoFlu, a quadrivalent seasonal flu vaccine, with an as-of-yet unapproved COVID-19 vaccine candidate called NVX-CoV2373.18 This COVID vaccine contains spike proteins produced by moth cells infected with a genetically engineered from the genetic sequence of the first strain of SARS-CoV-2.19,20
•A pneumococcal-COVID booster shot21 — This combo shot, made by Pfizer, is currently being tested on adults over 65 who have already been fully vaccinated against COVID-19. The shot combines the company’s pneumonia vaccine (pneumococcal conjugate vaccine) with a third dose of its current mRNA COVID-19 vaccine.
•mRNA seasonal influenza vaccines22 — The same mRNA technology used in Moderna’s and Pfizer’s COVID vaccines are now also being employed to develop seasonal flu vaccines. One advantage, from a production standpoint, is that such a vaccine can be developed in as little as one month. This would give researchers more time to determine which strains are in circulation that particular season.
We’re Speeding Toward Disaster
What no one is asking or talking about is what might happen if you instruct your body to continuously make spike proteins against several different types of viruses on a continuous basis, perhaps for years on end, if not the rest of your life.
No one knows just how long the cellular instructions remain viable as those studies have never been done. Even worse, they will not be keeping track of who was vaccinated and who wasn’t when people die, making it impossible to pin the blame on the vaccine.
Already, a growing list of physicians and scientists are warning that the COVID-19 shots may end up being a form of mass euthanasia. Many predict mass deaths among the vaccinated to occur within the next several years as their immune function breaks down and cardiovascular damage sets in. The idea that we’re going to add several gene therapy shots into an annual regimen will only exacerbate the predicted deaths.
Circling back to where we started, you can expect to see a new round of fear-mongering crop up as we head into fall and winter, this time badgering you to get your seasonal flu shot on top of the COVID-19 vaccine, plus a booster.
According to Moderna CEO Stephanie Bancel, those who got their first and second shots in December 2020 and January 2021 should prepare to get a third booster shot around September 2021.23 Pfizer CEO Albert Bourla has also stated that a booster may be required eight to 12 months after the initial two doses.24
Who knows, the way things are speeding along, perhaps NovaVax’s RNA-based COVID-flu combo shot will be ready for prime time by then too. I hate to be a pessimist, but I don’t foresee a happy ending to this trend. Your best bet is to take your time and don’t be so quick to offer up your body as a guinea pig for these gene-based injections. In time, the truth will become apparent, if it isn’t already.
Sources and References
- 1, 3 NBC News May 9, 2021
- 2 CDC Flu View Week 19 ending May 15, 2021
- 4 Scientific American April 29, 2021
- 5 Emerging Infectious Diseases May 2020; 26(5)
- 6 WHO.int
- 7 WHO.int Advice on the Use of Masks in the Context of COVID-19
- 8 medRxiv April 7, 2020 DOI: 10.1101/2020.03.30.20047217
- 9 JAMA 2009;302(17):1865-1871
- 10 BMJ Open 2015;5:e006577
- 11, 12 The Federalist October 29, 2020
- 13 Rochester First.com May 13, 2020
- 14 The Fat Emperor Data on Lockdown Weak Efficacy and Huge Harms
- 15 Preprints.org 2020: 2020100330 DOI: 10.20944/preprints202010.0330.v2
- 16 The Defender May 21, 2021
- 17 World Pharma News May 10, 2021
- 18 NVX-CoV2373 FDA Approval Status
- 19 Quartz December 28, 2020
- 20 The Guardian January 31, 2021
- 21 Reuters May 24, 2021
- 22 Washington Post April 11, 2021
- 23, 24 Business Insider May 20, 2021

